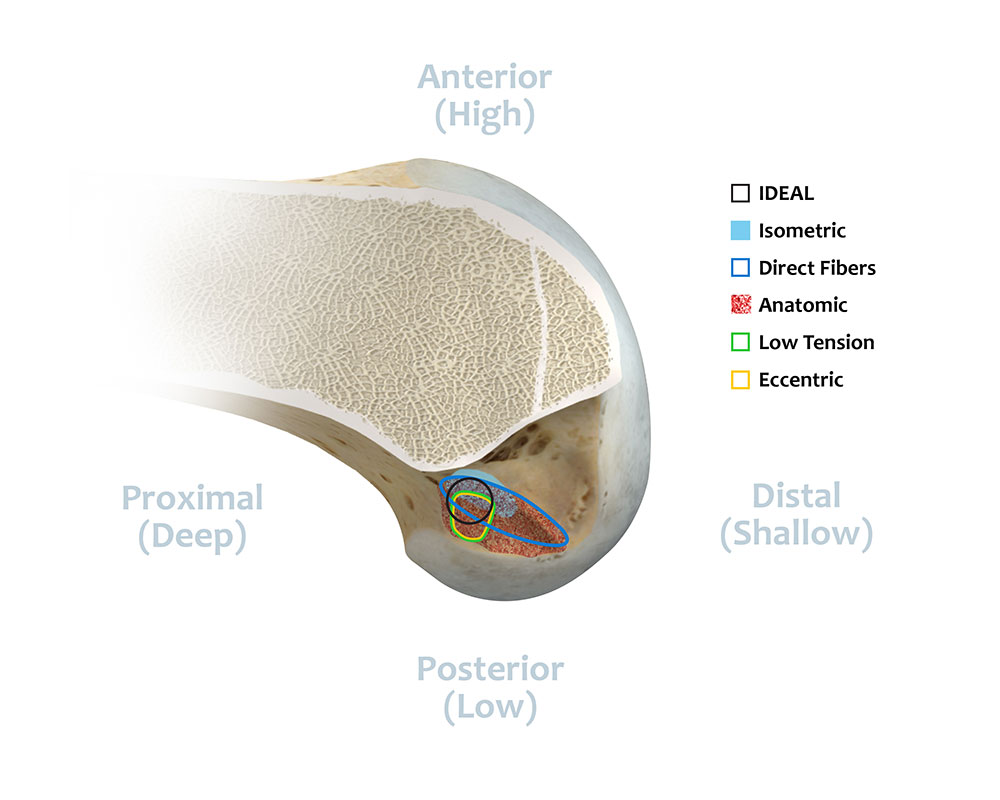
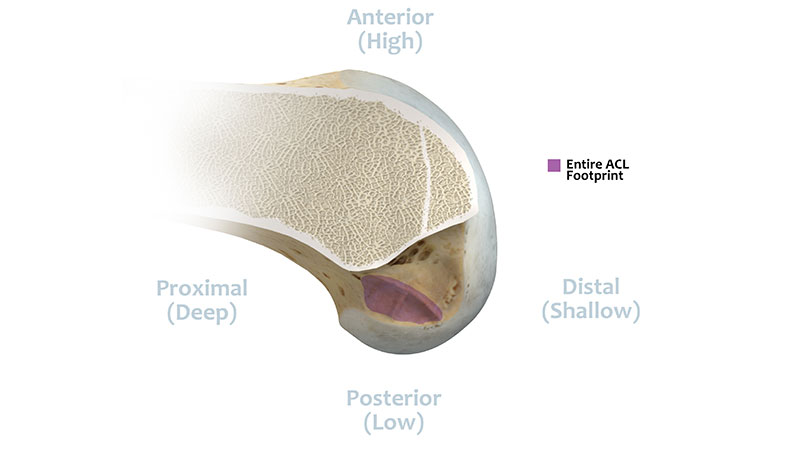
The I.D.E.A.L. Femoral Tunnel Location
Collectively, these three surgeons have 70 years of clinical and research experience in the field of ACL reconstruction. Working as a team they performed a comprehensive review of a large body of anatomic, histologic, biomechanical, and clinical data and recommend the use of the acronym 'I.D.E.A.L.' as an abbreviated nomenclature for describing the guidelines for placing the femoral tunnel.




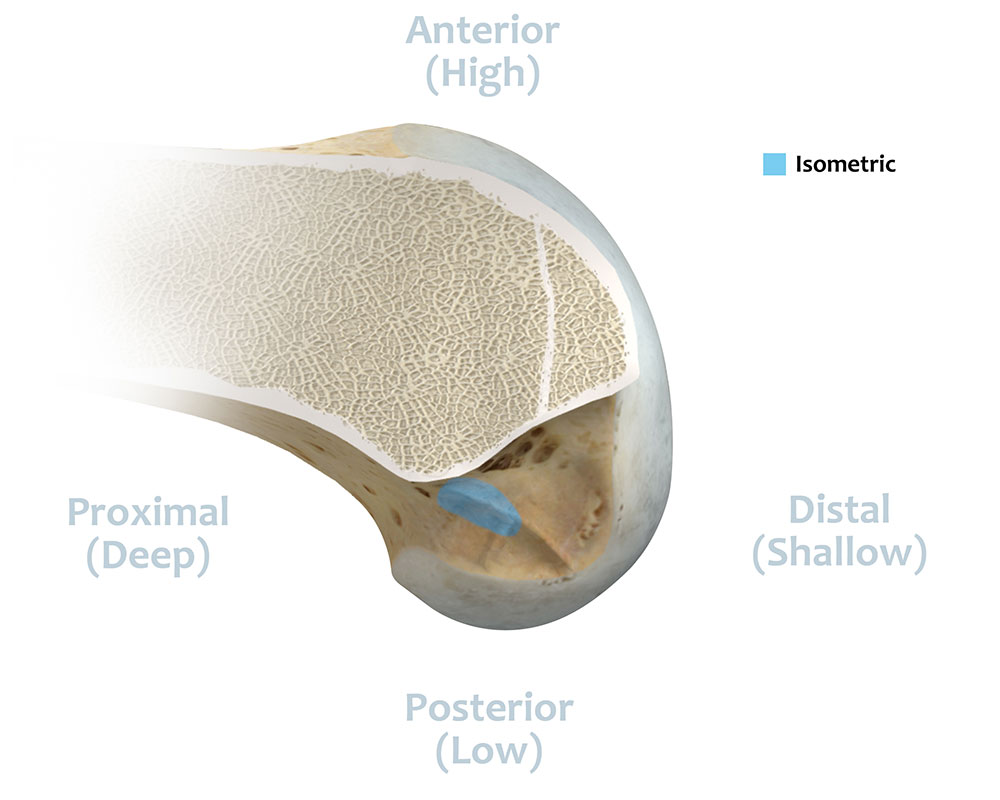
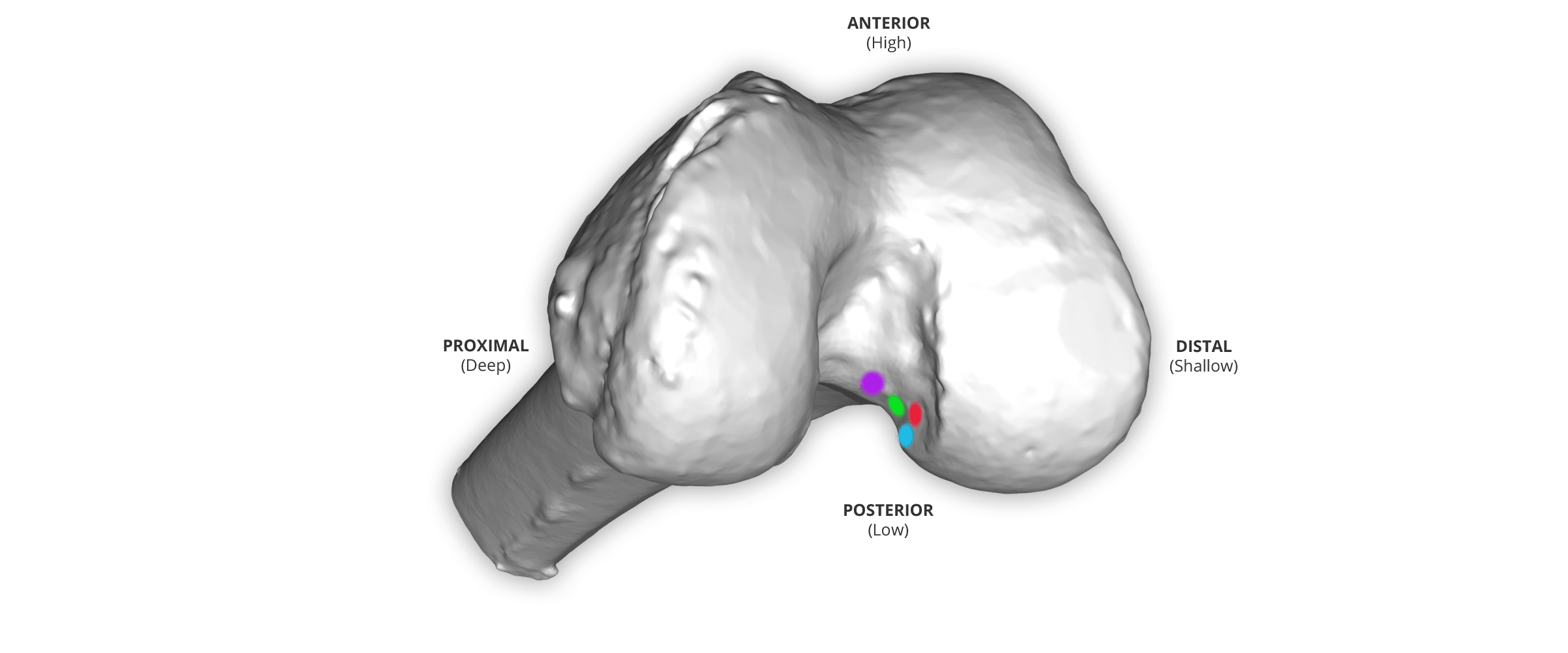
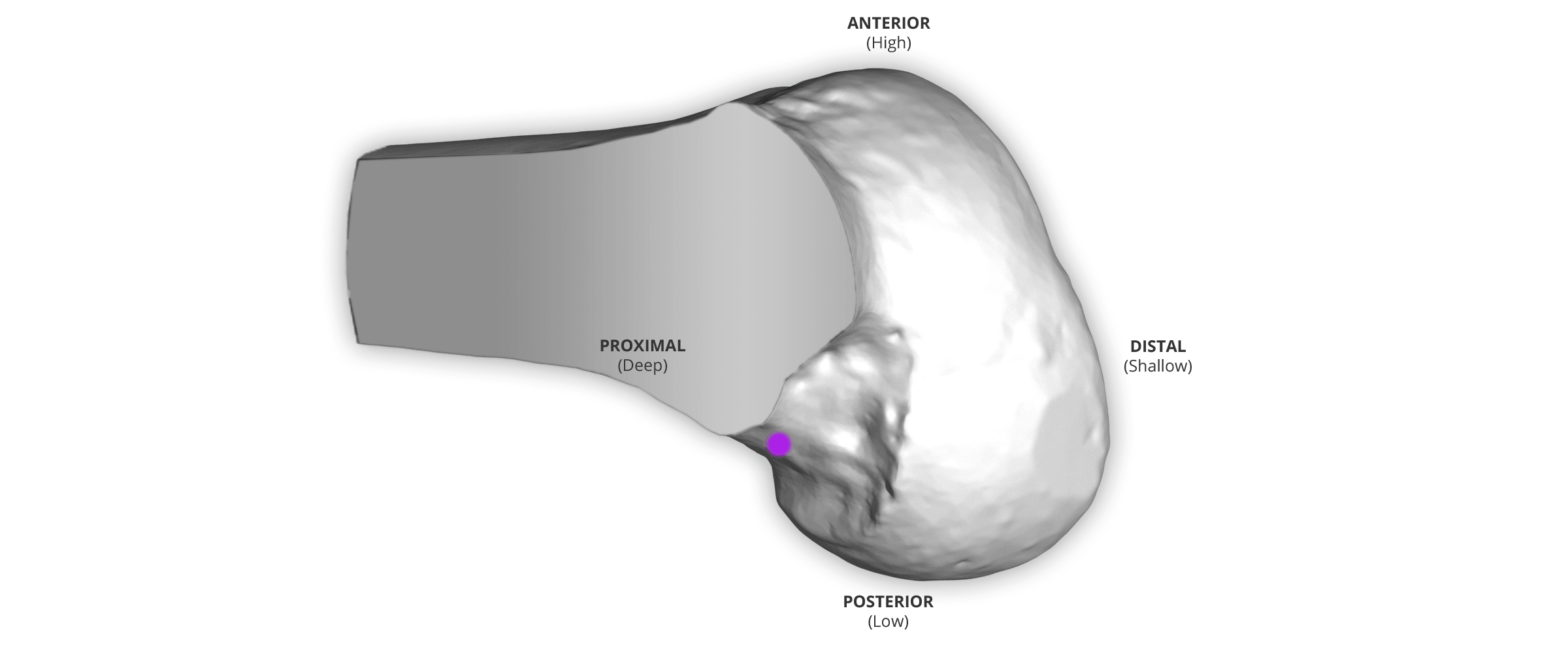
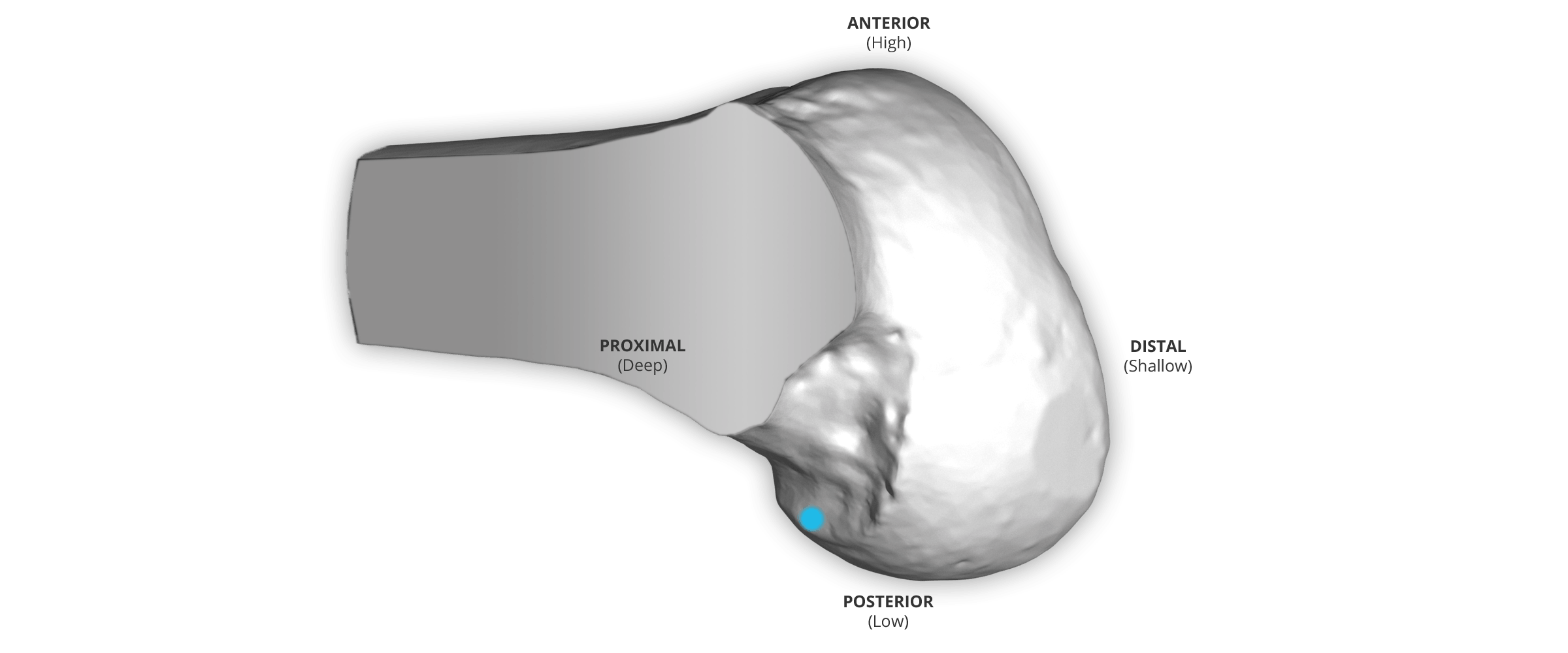
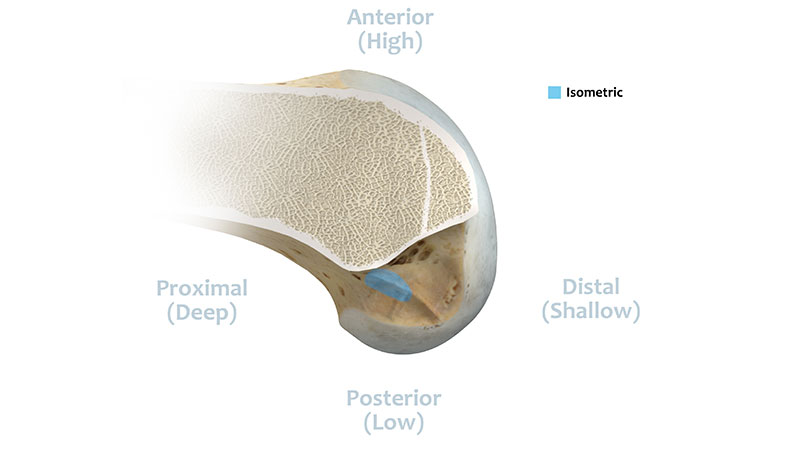
Isometric: Graft will have a length tension relationship that is similar to the native ACL.1,2,3
References
- Giron, Francesco: Femoral Attachment of the Anterior Cruciate Ligament. Knee Surg Sports Traumatol Arthrosc (2006) 14: 250-256.
- Zavras, T. D.; Race, A.; and Amis, A. A.: The Effect of Femoral Attachment Location on Anterior Cruciate Ligament Reconstruction: Graft Tension Patterns and Restoration of Normal Anterior-Posterior Laxity Patterns. Knee Surg Sports Traumatol Arthrosc, 13(2): 92-100, 2005.
- Simmons, R.; Howell, S. M.; and Hull, M. L.: Effect of the Angle of the Femoral and Tibial Tunnels in the Coronal Plane and Incremental Excision of the Posterior Cruciate Ligament on Tension of an Anterior Cruciate Ligament Graft: An in vitro Study. J Bone Joint Surg Am, 85-A(6): 1018-29, 2003.

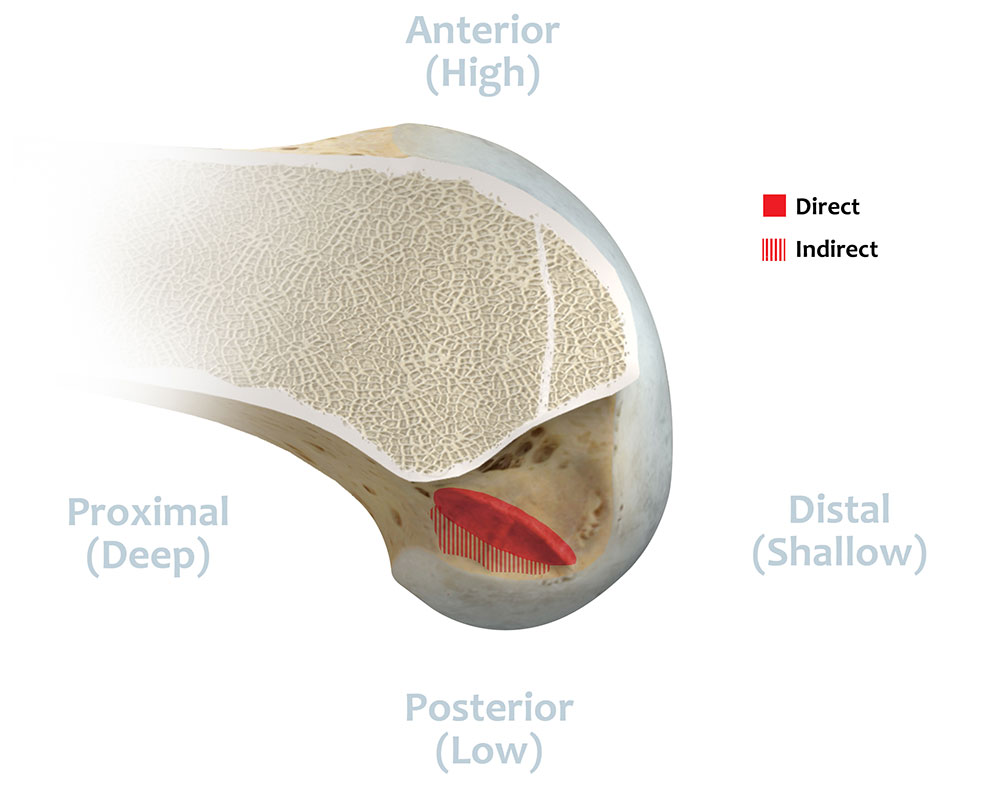
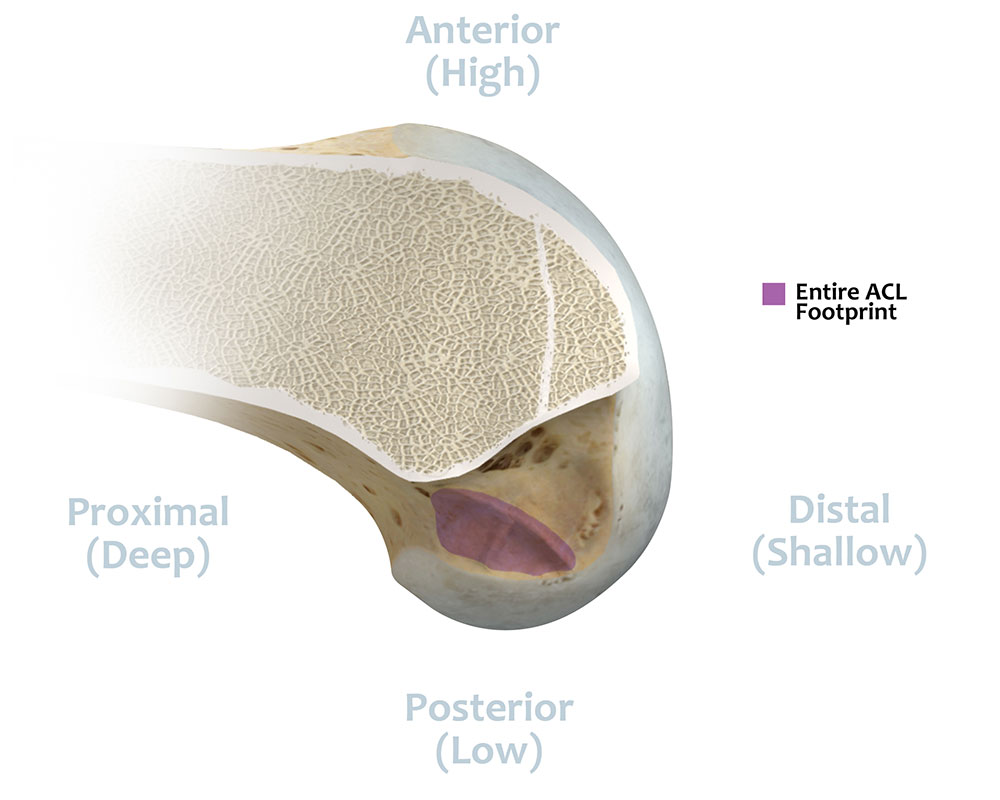
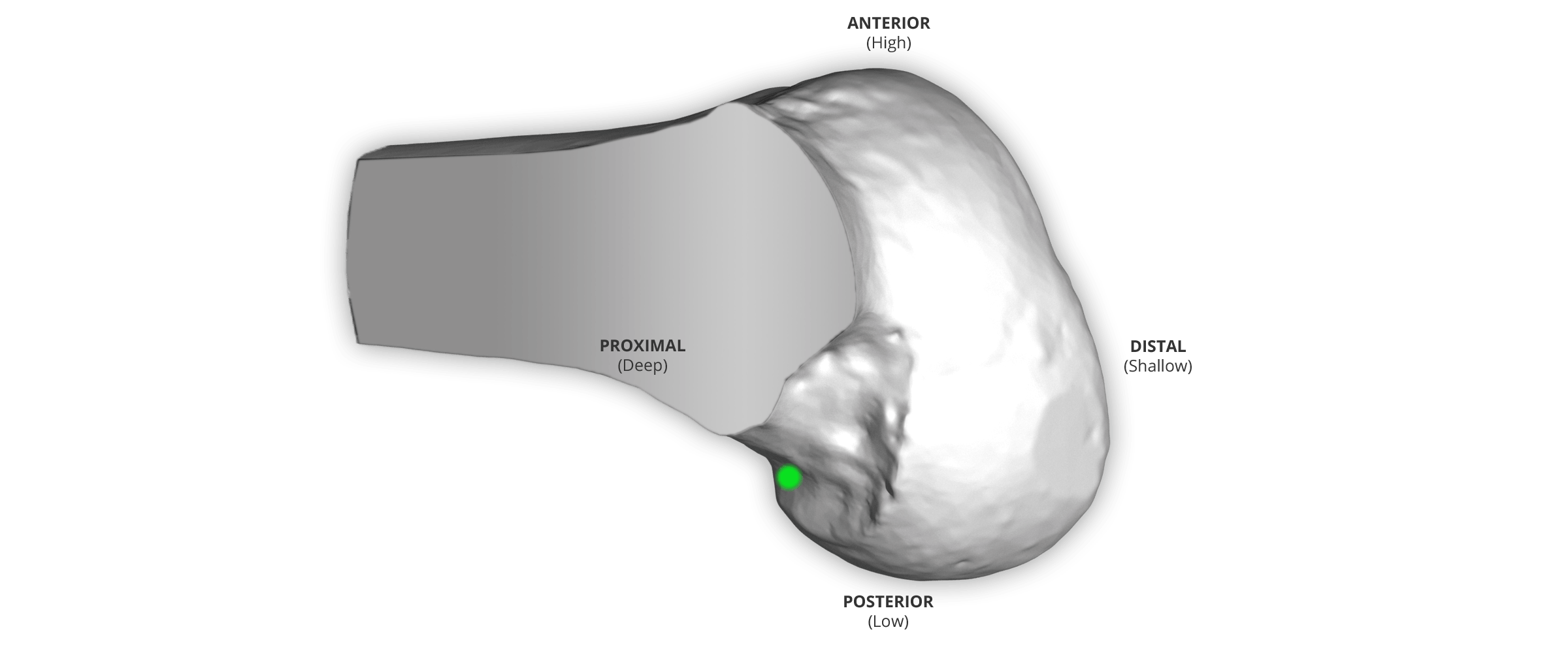
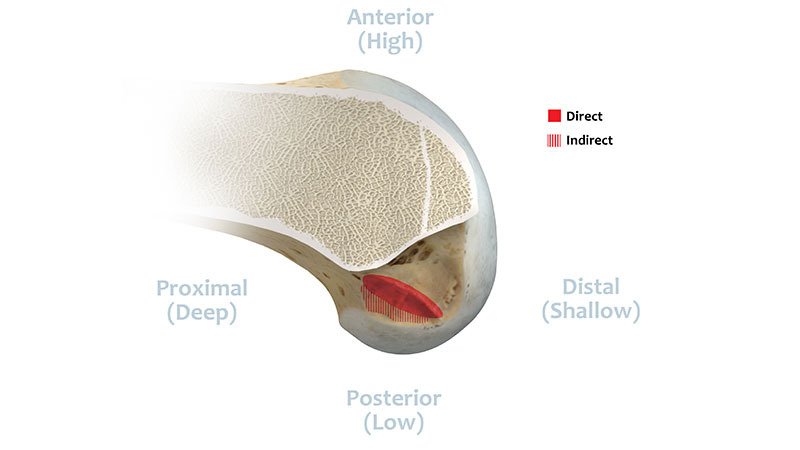
Direct Fibers: Fibers that have direct insertion on the footprint and fibers that are closest to the ridge.4
References
- Sasaki, Norihiro; Ishibaski, Yasuyuki ; Tsuda, Eiichi: Femoral Insertion of the Anterior Cruciate Ligament: Discrepancy Between Macroscopic and Histological Observations. Arthroscopy: The Journal of Arthroscopic and Related Surgery, Vol 28, No 8 (August), 2012: pp 1135-1146.

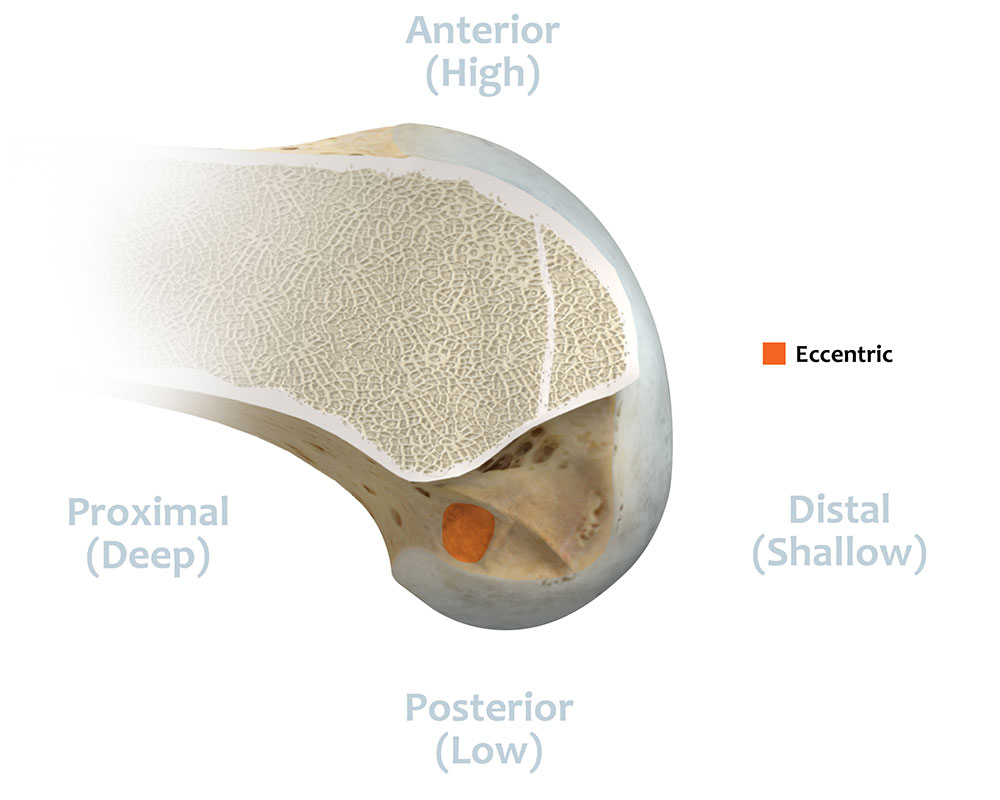
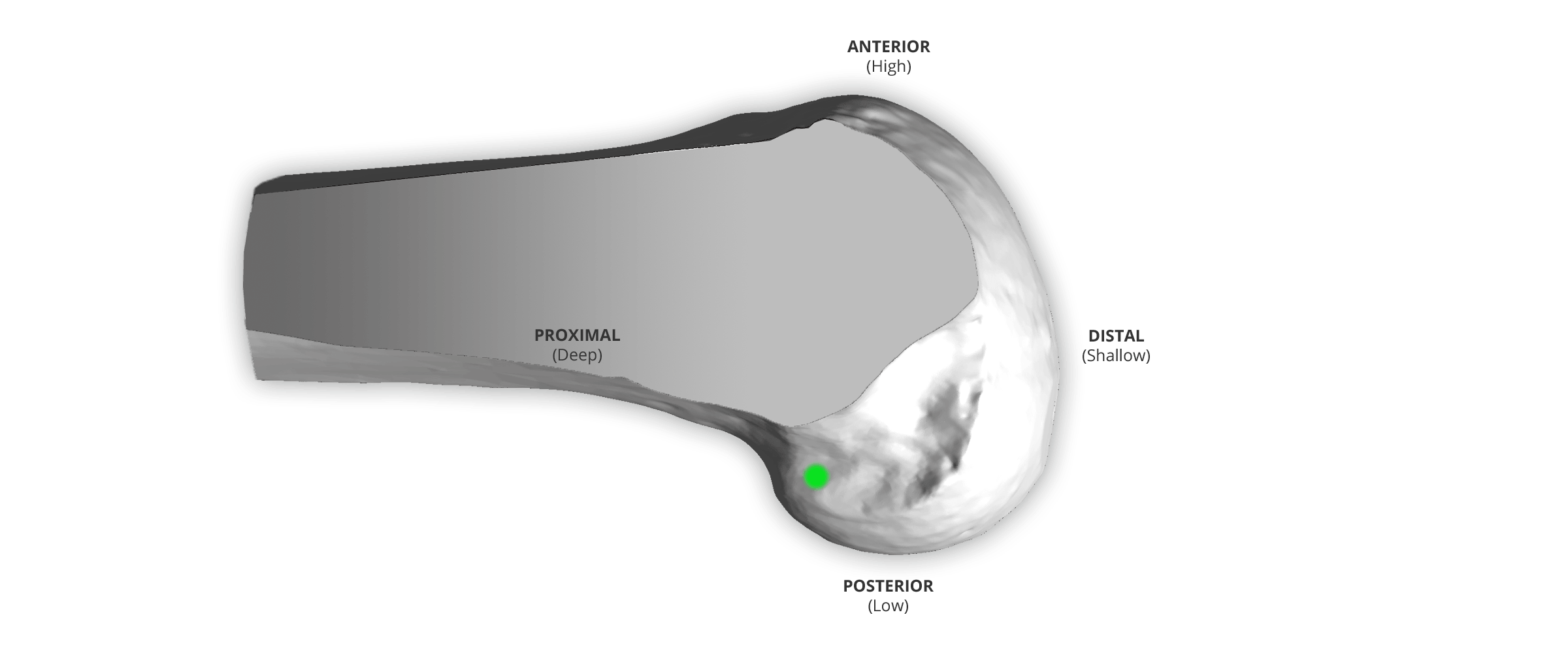
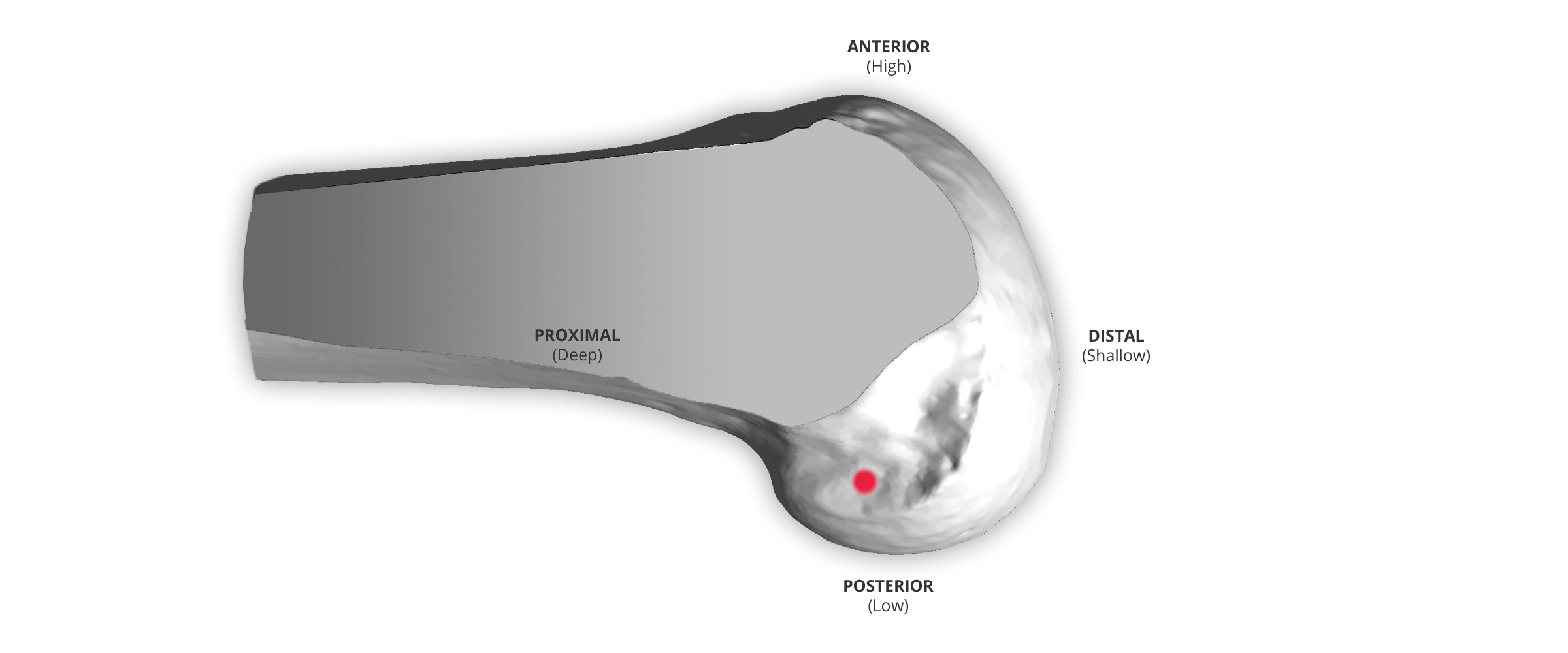
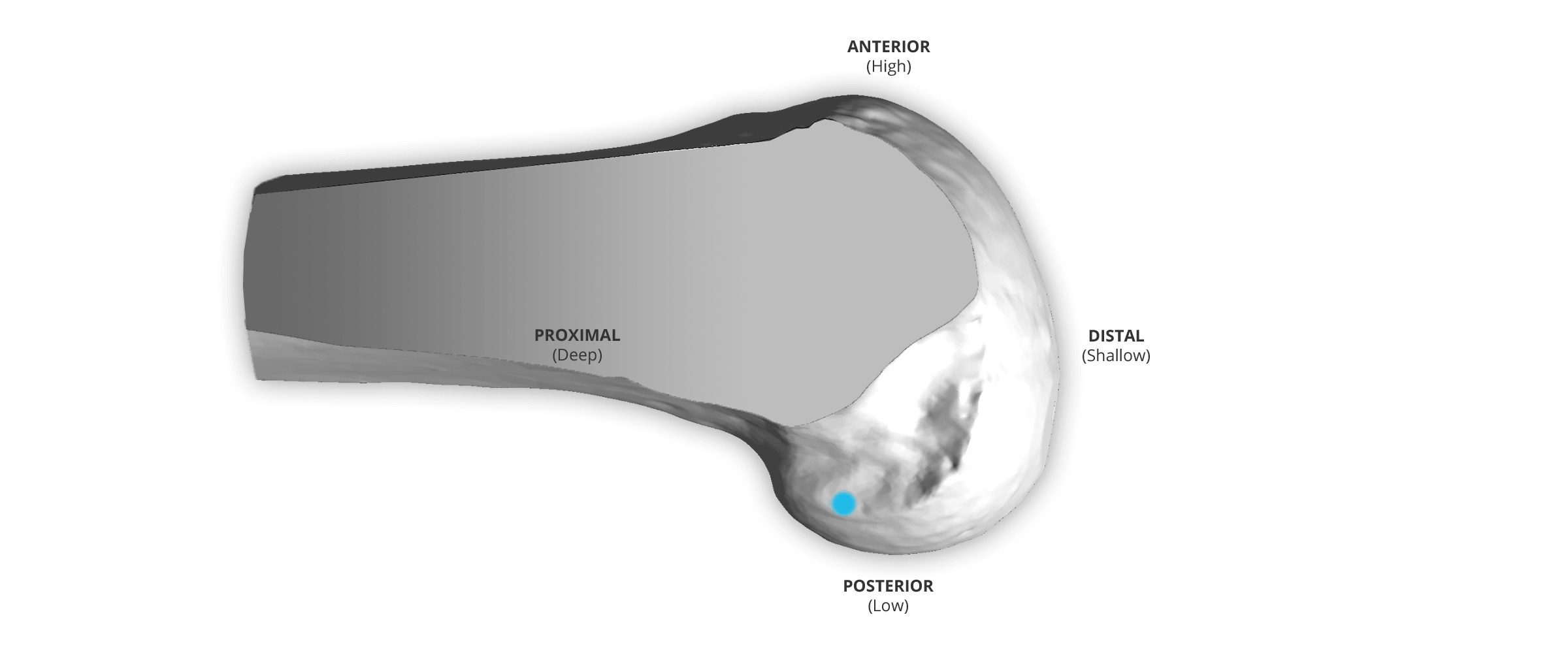
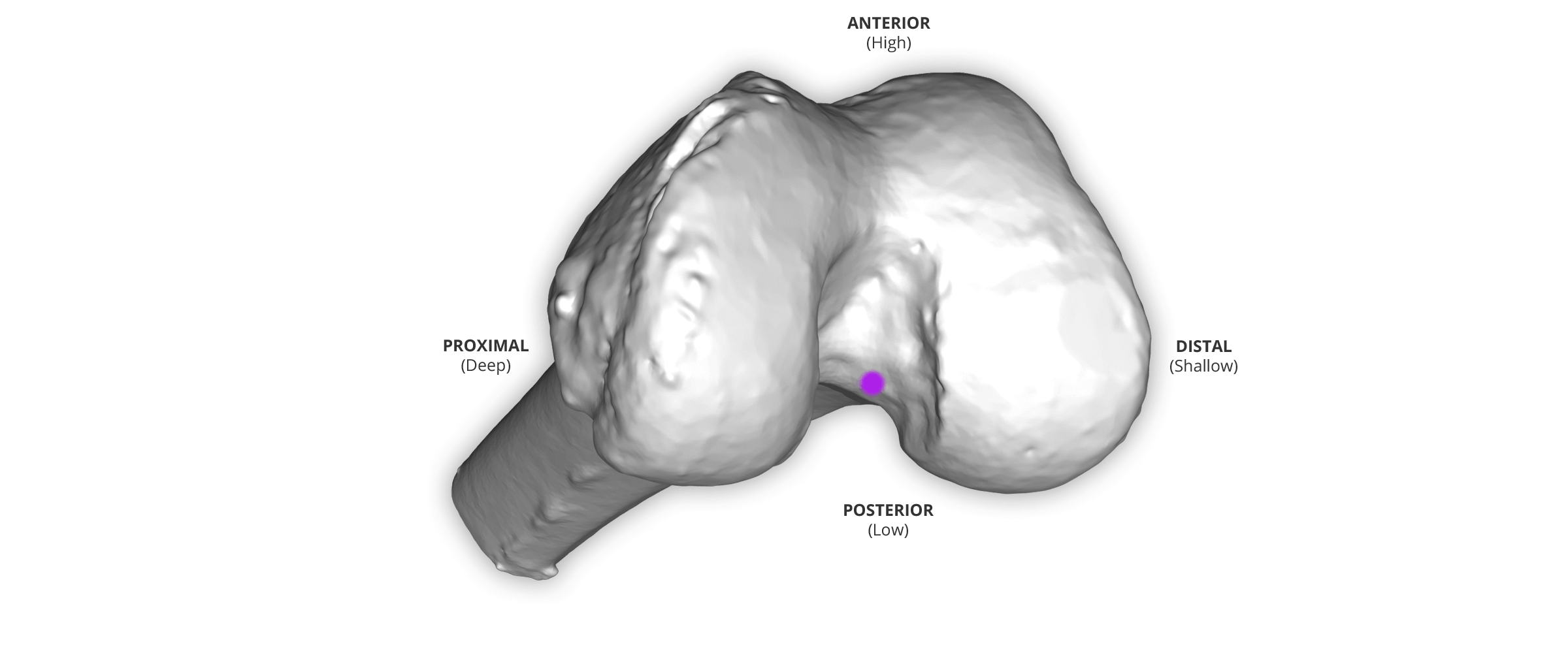
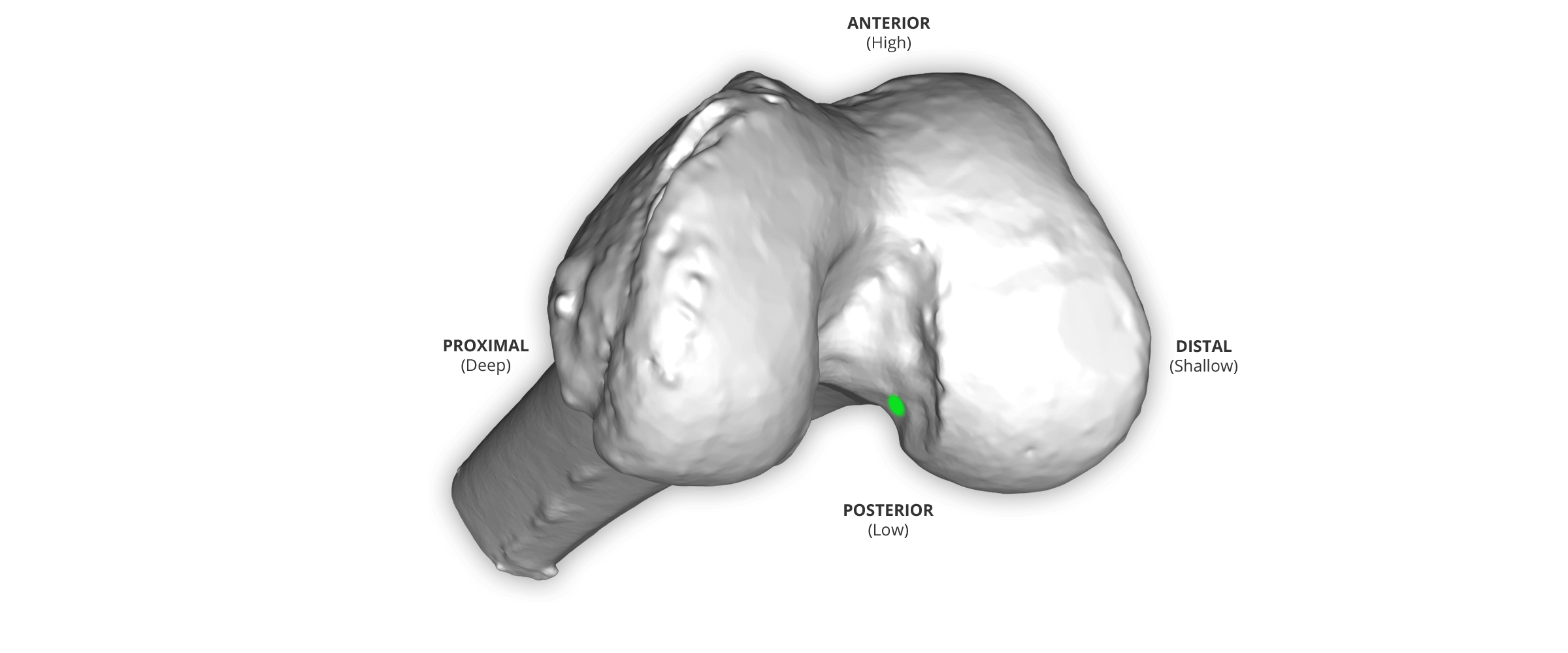
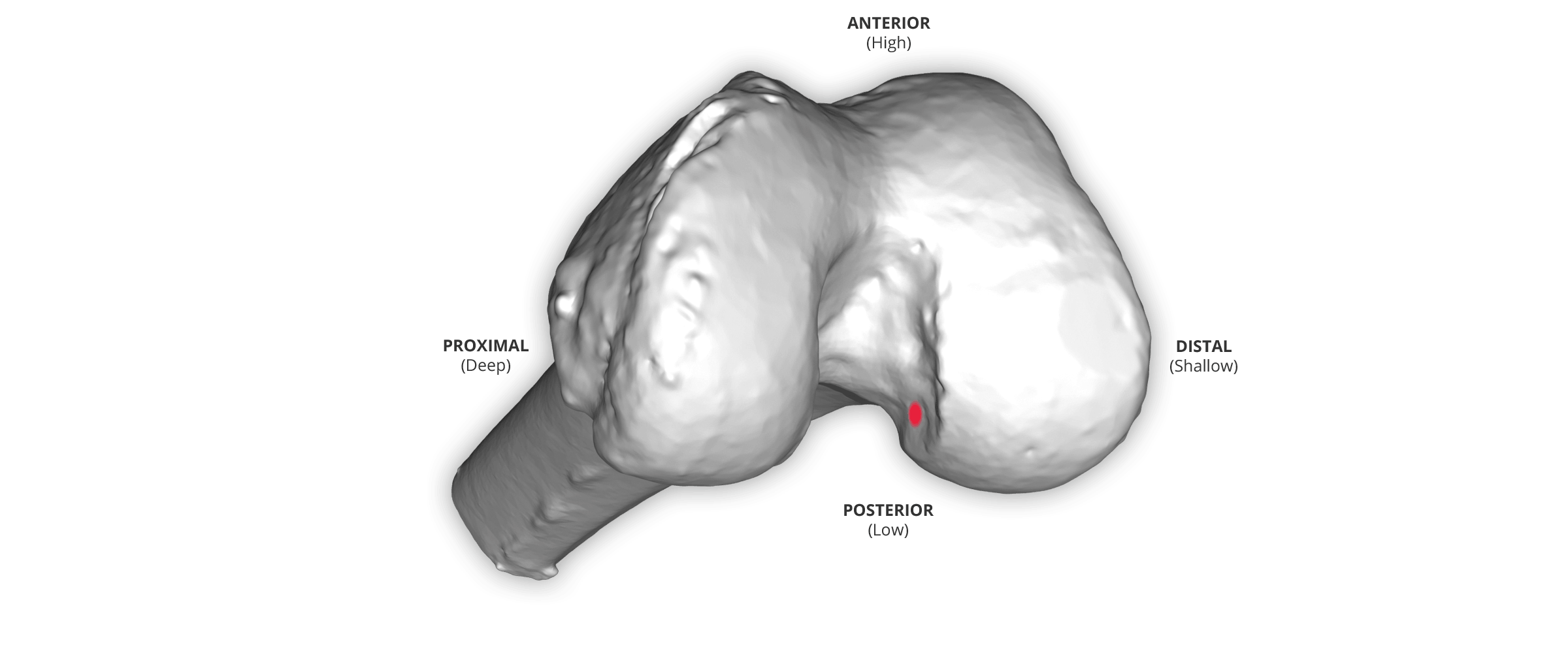
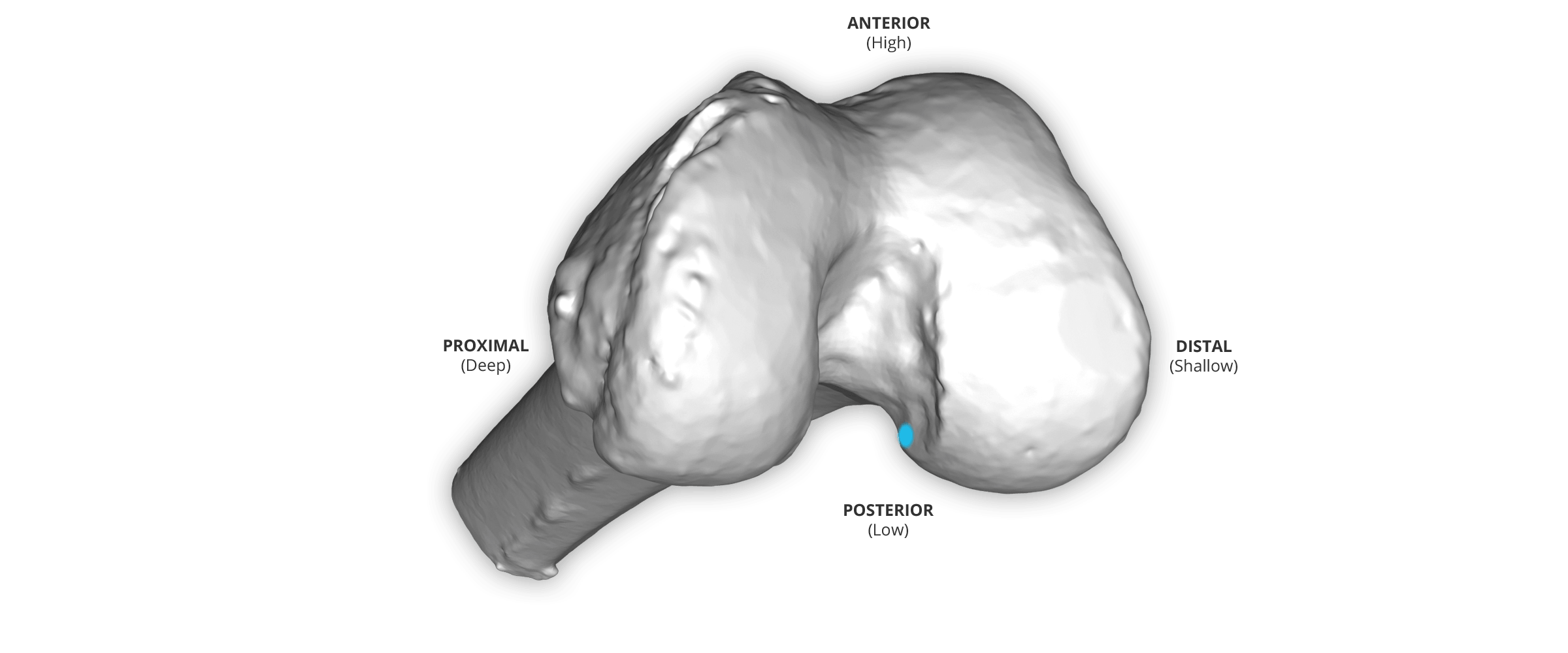
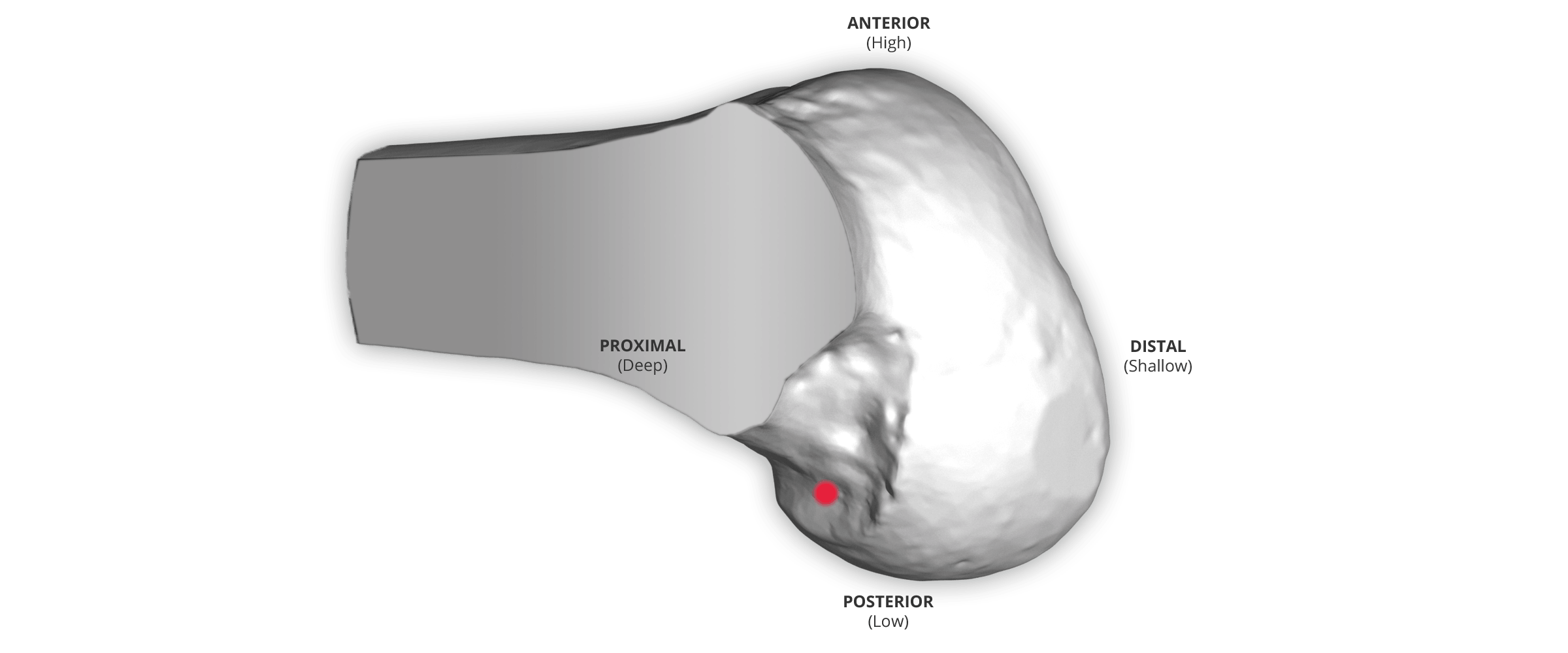
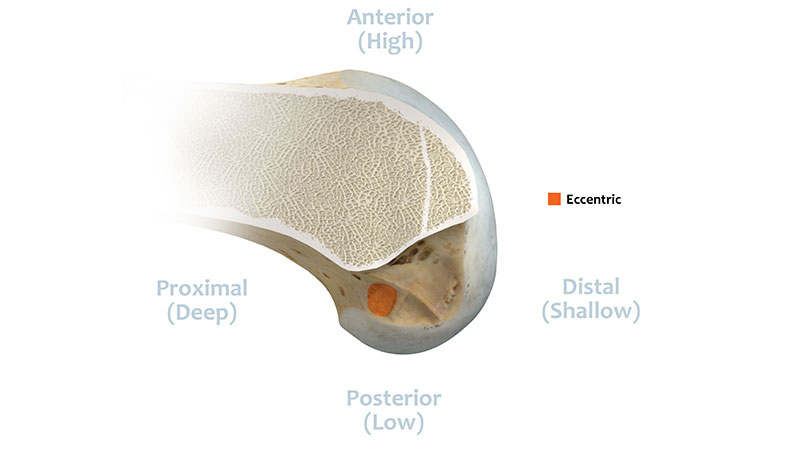
Eccentric: Anterior or higher in the footprint and in the anterior-medial portion of the ACL.5
References
- Howell, S.M.; Gittins, M.E.; Gottlieb, J.E.; Traina, S.M.; and Zoellner, T.M.: The Relationship between the Angle of the Tibial Tunnel in the Coronal Plane and Loss of Flexion and Anterior Laxity after Anterior Cruciate Ligament Reconstruction. American Journal of Sports Medicine, 29(5); 2001, pp 567-74.
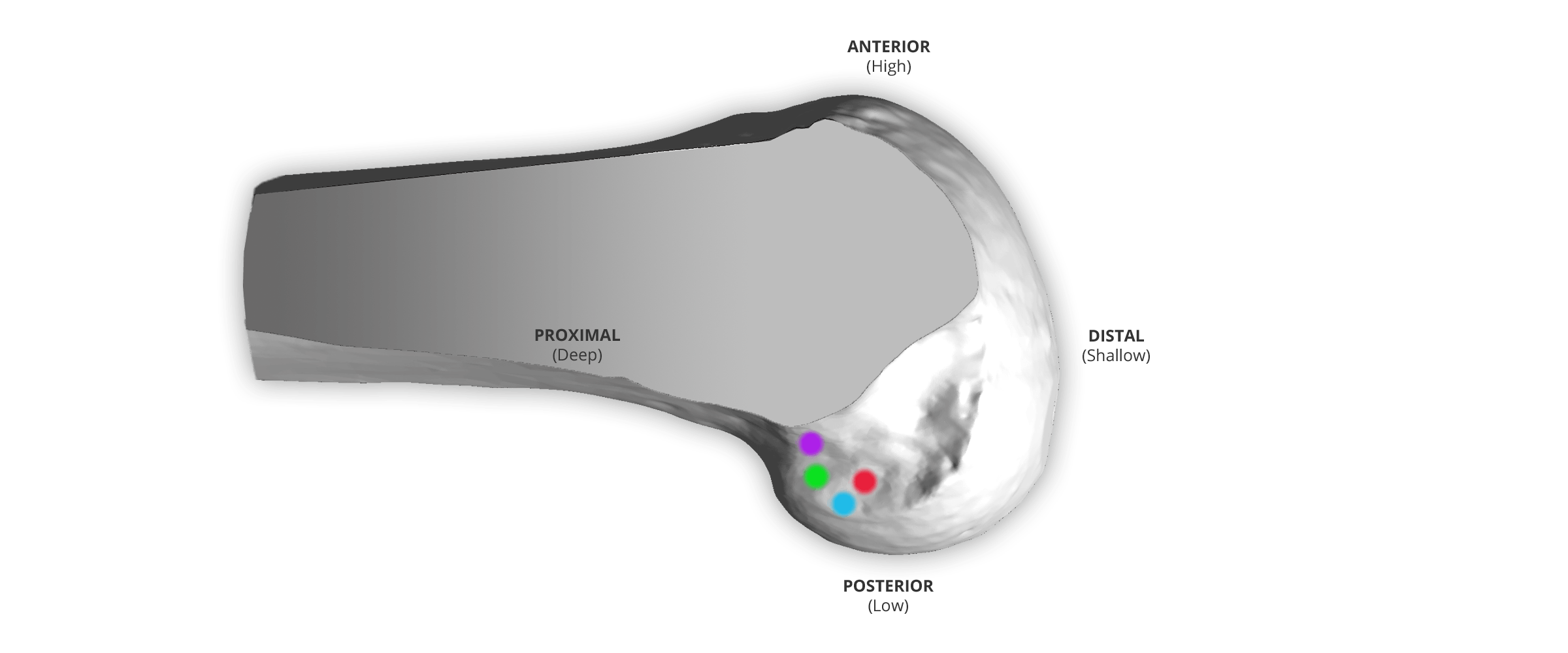
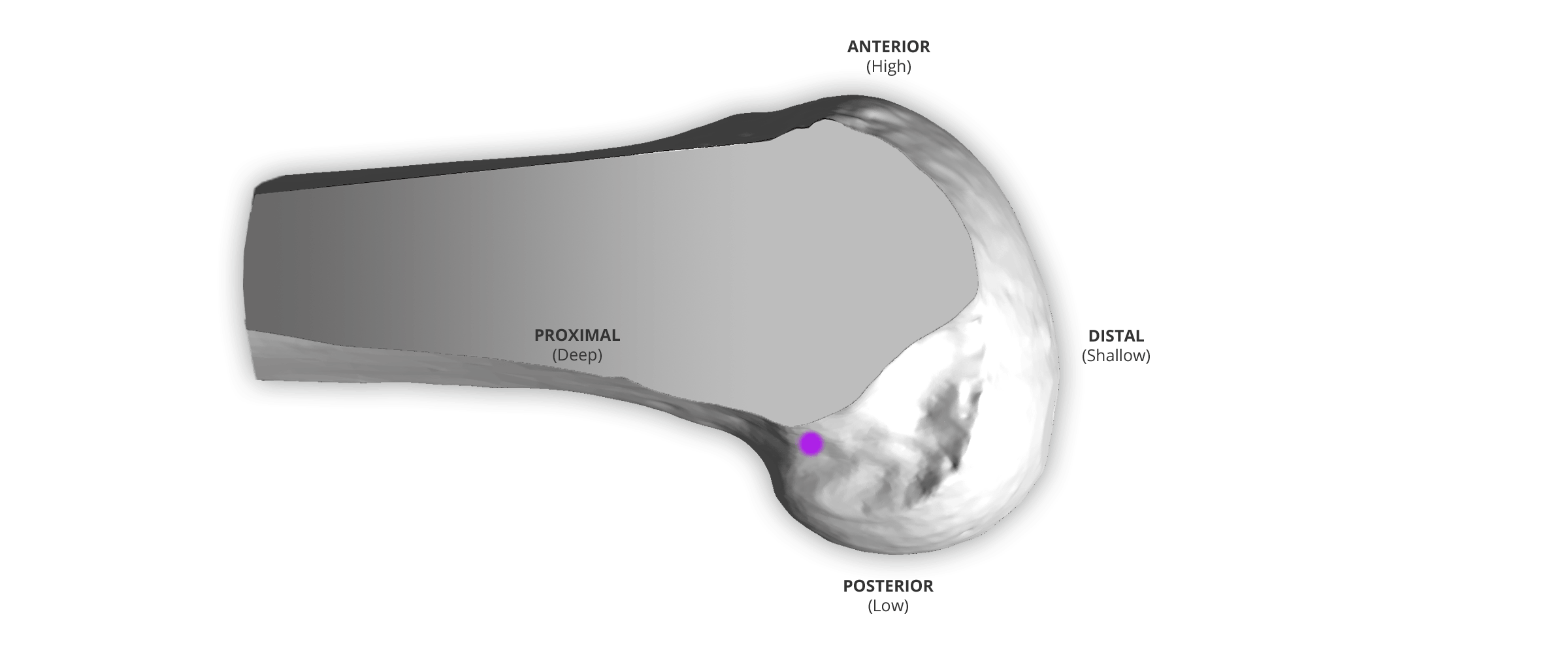
Equidistant: Halfway between the top and the bottom of the notch, which is the inter-operative checkpoint.3,6,7,8,9
References
- Simmons, R.; Howell, S. M.; and Hull, M. L.: Effect of the Angle of the Femoral and Tibial Tunnels in the Coronal Plane and Incremental Excision of the Posterior Cruciate Ligament on Tension of an Anterior Cruciate Ligament Graft: An in vitro Study. J Bone Joint Surg Am, 85-A(6): 1018-29, 2003.
- Markolf, K. L.; Park, S.; Jackson, S. R.; and McAllister, D. R.: Anterior-Posterior and Rotatory Stability of Single and Double-Bundle Anterior Cruciate Ligament Reconstructions. J Bone Joint Surg Am, 91(1): 107-18, 2009.
- Markolf, K. L.; Park, S.; Jackson, S. R.; and McAllister, D. R.: Contributions of the Posterolateral Bundle of the Anterior Cruciate Ligament to Anterior-Posterior Knee Laxity and Ligament Forces. Arthroscopy. The Journal of Arthroscopic and Related Surgery, VOL 24, No 7 (July), 2008: pp 805-809.
- Markolf, K. L.; Park, S.; Jackson, S. R.; and McAllister, D. R.: A Comparison of 11 O'clock Versus Oblique Femoral Tunnels in the Anterior Cruciate Ligament-Reconstructed Knee. The American Journal of Sports Medicine, Vol. 38, No. 5.
- Rahr-Wagner, L. R.: Increased Risk of Revision After Anteromedial Compared With Transtibial Drilling of the Femoral Tunnel During Primary Anterior Cruciate Ligament Reconstruction. Results from the Danish Knee Ligament Reconstruction Register. Arthroscopy: The Journal of Arthroscopic and Related Surgery, 29(1); (January), 2013: pp 98-105.

Anatomic: Fibers within the bounds of the native ACL graft, which is anterior (higher) than the indirect fibers.4,10
References
- Sasaki, Norihiro; Ishibaski, Yasuyuki ; Tsuda, Eiichi: Femoral Insertion of the Anterior Cruciate Ligament: Discrepancy Between Macroscopic and Histological Observations. Arthroscopy: The Journal of Arthroscopic and Related Surgery, Vol 28, No 8 (August), 2012: pp 1135-1146.
- Morgan, Joseph A.: Femoral Tunnel Malposition in ACL Revision Reconstruction. J Knee Surg. 2012 November; 25(5): 361-368.

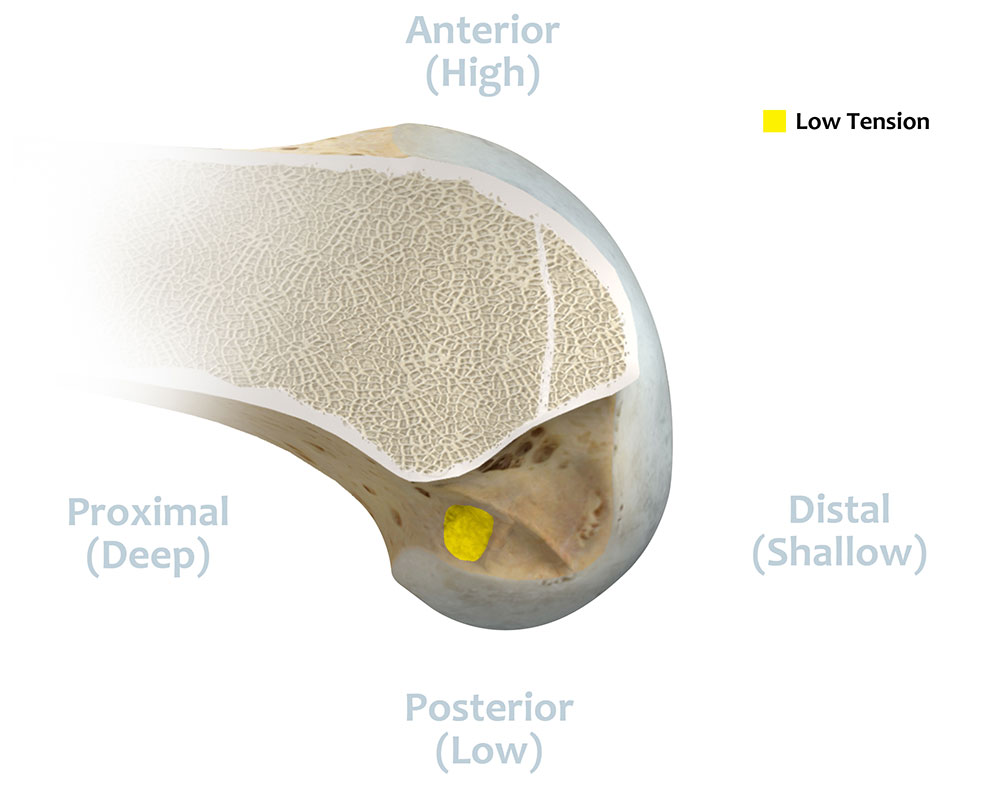
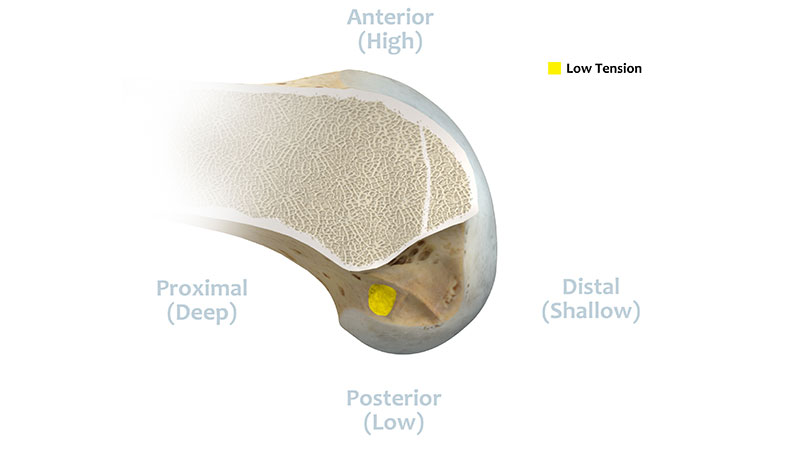
Low Tension: Tension of the native ACL should match the low tension-flexion pattern of the native ACL.2,3,6
References
- Zavras, T. D.; Race, A.; and Amis, A. A.: The Effect of Femoral Attachment Location on Anterior Cruciate Ligament Reconstruction: Graft Tension Patterns and Restoration of Normal Anterior-Posterior Laxity Patterns. Knee Surg Sports Traumatol Arthrosc, 13(2): 92-100, 2005.
- Simmons, R.; Howell, S. M.; and Hull, M. L.: Effect of the Angle of the Femoral and Tibial Tunnels in the Coronal Plane and Incremental Excision of the Posterior Cruciate Ligament on Tension of an Anterior Cruciate Ligament Graft: An in vitro Study. J Bone Joint Surg Am, 85-A(6): 1018-29, 2003.
- Markolf, K. L.; Park, S.; Jackson, S. R.; and McAllister, D. R.: Anterior-Posterior and Rotatory Stability of Single and Double-Bundle Anterior Cruciate Ligament Reconstructions. J Bone Joint Surg Am, 91(1): 107-18, 2009.
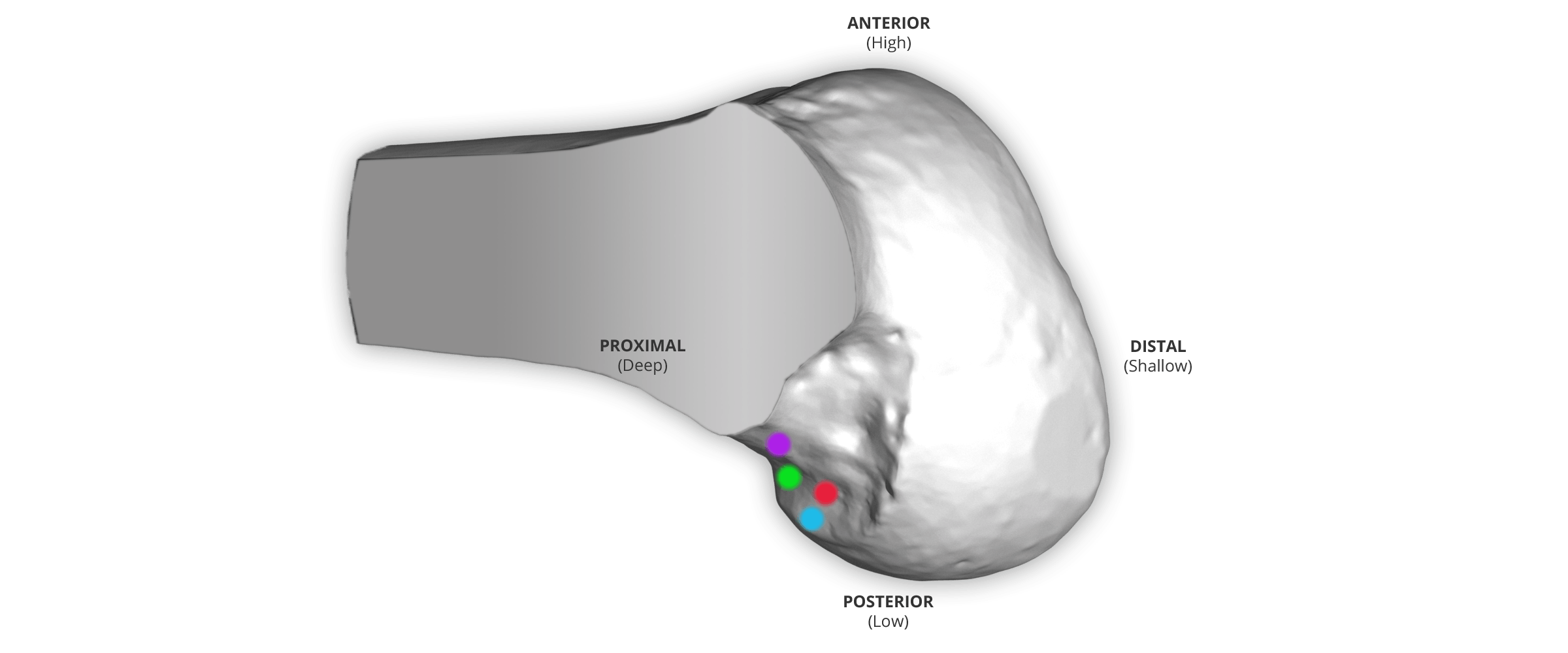
Evidence suggests that the I.D.E.A.L. femoral tunnel position should: 1) replicate the most Isometric fibers within the native ACL, 2) be localized in the Direct fiber subsection of the ACL origin based on histology, 3) be placed Equidistantly from the bottom and top of the notch with a tunnel backwall that is 1 mm thick and Eccentrically located high and deep within the footprint, 4) be Anatomic in that the ACL graft is within the native ACL origin, and 5) achieve a Low tension-flexion pattern in the ACL graft that replicates the tension-flexion behavior of the native ACL.
Surgeon Development Team
- Stephen Howell, MD
- Andrew Pearle, MD
- David McAllister, MD